BACKGROUND
AAA is more common than you would think, being present in 2-4% of folks over 50. When identified, they can be followed conservatively by a surgeon, but ruptures carry an 80% mortality rate. Point of care ultrasound can quickly identify AAA in the appropriate patient. Computed tomography has near 100% accuracy for the diagnosis of AAA. Ultrasound is not far off with accuracy of 97-100%, and can be performed quickly, at the point of care, with no exposure to ionizing radiation, nor iv contrast.

INDICATIONS
Ultrasound is the ideal modality to quickly assess for abdominal aortic disease with a reported sensitivity of 100% and specificity 98-100%. Point of care ultrasound has been shown not only to be fast and accurate but to significantly decrease time to diagnosis. Consider a quick point-of-care ultrasound, especially in the older population, for any patient with:
- adominal pain
- abdominal mass
- flank pain
- back pain
- shock / hypotension
- syncope
PREPARATION and POSITIONING
The patient should be supine. This may be difficult as the pain of a rupturing aneurysm is frequently unaffected by a change in position, so patients will writhe as they do with kidney stones, a frequent initial misdiagnosis.
The large curvilinear “abdominal” probe is used. A lower frequency (1-5 MHz) probe will give you better penetration at the expense of resolution.
VIEWS
Place the probe in a transverse orientation below the xiphoid process and scan down the abdomen, stopping to obtaining the following views: proximal aorta, mid-aorta, distal aorta, the bifurcation of the iliacs and then a longitudinal view of the aorta.

Proximal / Upper Aorta


Mid Aorta
Distal / Lower Aorta
Aortic Bifurcation and Iliacs
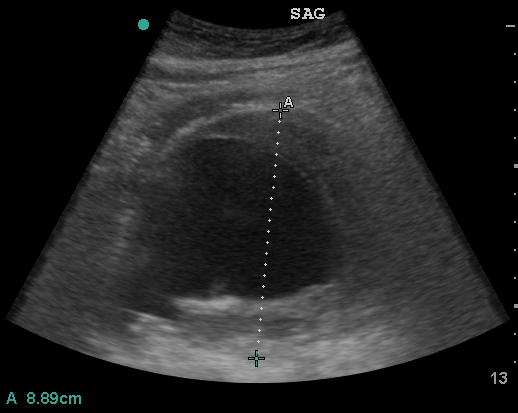
Longitudinal View of Aorta
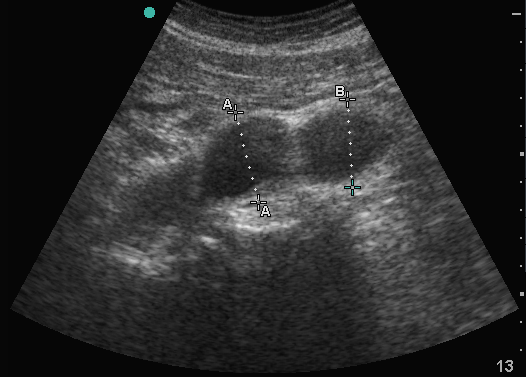
MEASURING THE AORTA
The Abdominal aorta is always measured in transverse. This minimizes the possibility of underestimating the size of the aorta. Our goal is to be sensitive for AAA, so we aim to overestimate the size of the aorta. In this vein, we don’t measure the diameter between inner walls, instead placing our caliper points on the outer walls of the aorta.
The normal aorta will measure less than 2 cm. An aorta > 3 cm in size is aneurysmal. Candidacy for surgical management varies by surgical experience and volume but most use an aneurysm size > 5 cm as an indication for repair.
This concept applies to measurement of the Iliacs as well. We measure in transverse from outer to outer wall. Normal Iliac arteries are < 1.5 cm in size with > 3 cm being abnormal.
PITFALLS
Intestinal gas

One of the most common difficulties when scanning the aorta is the presence of bowel gas. A technique of graded compression which entails the application of gradual continuous pressure will move the interposed gas aside, allowing visualization of the structures of interest – in this case the abdominal aorta.
Other pitfalls include: confounding IVC with aorta, not measuring in transverse axis, and not measuring outer wall to outer wall.
PATHOLOGY
AORTIC DISSECTION
RESOURCES AND REFERENCES
- Sonoguide AAA chapter
- Shanzer A, Oderich GS. Management of Abdominal Aortic Aneurysm. NEJM 385;18. October 28, 2021.